
Regulation of the Heartbeat
Regulation of the Heartbeat (Myogenic, Neural & Hormonal) Official Links Instagram Youtube Jki-discord Notes & Illustrations Quizzes Summary & Transcript 📢 Currently, there is no PDF for this video.If you’re interested in having one, feel free to send an inquiry, and I may create it in the future. BUT! There’s a quiz available in the next tab. 12345678910 Regulation of the Heartbeat – QUIZ Test your understanding with 10 random multiple-choice questions from the question bank. You're in the preview mode. Note: All elements work correctly on the front end. 1 / 10 What happens to stroke volume during an increase in venous return? A) Increases stroke volume B) Reduces stroke volume C) Stabilizes preload D) Decreases end-diastolic volume Increased venous return raises end-diastolic volume, enhancing stroke volume via the Frank-Starling mechanism. 2 / 10 How does myogenic regulation maintain cardiac function? A) Neural input adjustments B) Changes in afterload C) Hormonal feedback D) Intrinsic stretch-based regulation Myogenic regulation involves cardiomyocytes’ intrinsic ability to autoregulate contraction strength based on stretch. 3 / 10 What mechanism reduces cardiac output at extremely high HR? A) Enhanced preload B) Increased afterload C) Decreased filling time D) Stronger ventricular contraction At very high HR, insufficient ventricular filling time decreases stroke volume and cardiac output. 4 / 10 What effect does an increase in afterload have on stroke volume? A) Decreases stroke volume B) Increases stroke volume C) Stabilizes contractility D) Enhances preload Increased afterload decreases stroke volume as the heart works harder to overcome resistance, reducing ejection. 5 / 10 What role does the renin-angiotensin-aldosterone system (RAAS) play in cardiac regulation? A) Reduces preload B) Modulates parasympathetic activity C) Increases BP and CO D) Enhances HR RAAS increases blood pressure and CO by promoting vasoconstriction and sodium/water retention. 6 / 10 What is the role of natriuretic peptides in regulating blood volume and pressure? A) Enhance afterload B) Stabilize HR C) Reduce blood volume and pressure D) Increase preload Natriuretic peptides promote sodium and water excretion, reducing blood volume and pressure. 7 / 10 What effect does acetylcholine have on the pacemaker cells of the heart? A) Enhances depolarization B) Hyperpolarizes cells C) Activates ion influx D) Increases contractility Acetylcholine hyperpolarizes pacemaker cells, reducing HR and conduction velocity. 8 / 10 What effect does the Bowditch effect (staircase effect) have on cardiac output? A) Reduces stroke volume B) Inhibits calcium influx C) Enhances contractility D) Reduces HR It enhances contractility during increased HR due to improved calcium handling in cardiomyocytes. 9 / 10 Which ion is most responsible for increasing contractility during hypercalcemia? A) Calcium B) Magnesium C) Potassium D) Sodium Calcium increases myocardial contractility and shortens the QT interval. 10 / 10 How does sympathetic stimulation affect the refractory period of cardiomyocytes? A) Inhibits calcium influx B) Shortens refractory period C) Stabilizes contraction cycle D) Prolongs refractory period Sympathetic stimulation shortens the refractory period, allowing for faster contraction rates. Your score is The average score is 0% Description Complete Cheat Code for Heart Physiology Series: 1st Video: Types of cardiac muscle, action potentials of pacemaker cells and contractile myocardium, and general properties of cardiomyocytes. 2nd Video: Detailed exploration of the cardiac cycle, including phase-by-phase events, valve operations, and pressure differences. 3rd Video: Cardiac output. 4th Video: Regulation of heartbeat. Key Concepts Covered: 1. Overview of Cardiac Output (CO): Formula: CO = Heart Rate (HR) × Stroke Volume (SV). Regulation affects pacemaker activity or myocardial contraction. 2. Regulation Categories: Myogenic Regulation: Heterometric Regulation: Frank-Starling Mechanism: Increased end-diastolic volume (EDV) stretches cardiomyocytes, enhancing contraction and increasing SV. Homeometric Regulation: Bowditch Effect (Staircase Effect): Increased HR strengthens contractions due to enhanced calcium handling in cells. Neural Regulation: Involves the nervous system, divided into extracardiac and intracardiac regulation. Extracardiac Regulation: Sympathetic Nervous System: Increases HR, contractility, and CO via norepinephrine and epinephrine acting on β1-adrenergic receptors. Activates ion channels to enhance calcium influx, increasing contraction strength and speed. Parasympathetic Nervous System: Reduces HR and conduction velocity via acetylcholine on muscarinic receptors. Inhibits adenylyl cyclase, decreasing cAMP levels and activating K+ channels to hyperpolarize the membrane. Medullary Control: Integrates input from baroreceptors and chemoreceptors to modulate autonomic nervous system activity. Intracardiac Regulation: Intramural ganglia modulate cardiac function independent of direct CNS control. Humoral Regulation: Involves hormones in the blood influencing HR, contractility, and CO. Epinephrine: Released by adrenal medulla, activating β1-adrenergic receptors. Renin-Angiotensin-Aldosterone System (RAAS): Angiotensin II increases contractility, vasoconstriction, and blood volume. Aldosterone promotes sodium and water reabsorption, increasing blood pressure and CO. Thyroid Hormones (T3): Increase HR and contractility by influencing gene expression and ion channel activity. Glucocorticoids: Enhance myocardial contractility and adrenergic receptor sensitivity. Natriuretic Peptides (ANP, BNP): Reduce blood volume and pressure by promoting sodium and water excretion. 3. Ion Regulation: Calcium: Hypercalcemia increases contractility, shortening the QT interval. Hypocalcemia decreases contractility, prolonging the QT interval. Potassium: Hyperkalemia depolarizes cells, increasing arrhythmia risk. Hypokalemia reduces excitability, making depolarization more difficult. By understanding these regulatory mechanisms, you’ll gain a comprehensive understanding of how the body maintains cardiac function under various physiological conditions. #cardiacphysiology #heartfunction #extracardiac #ecg #medicaleducation #usmlepreparation #nursingeducation #premed #heartanatomy Sources: University lectures and notes Barrett, K. E., Barman, S. M., Boitano, S., & Brooks, H. L. (2016). Ganong’s Review of Medical Physiology (25th ed.). McGraw-Hill Education. Hall, J. E. (2016). Guyton and Hall Textbook of Medical Physiology (13th ed.). Elsevier. Mohrman, D. E., & Heller, L. J. (2014). Cardiovascular Physiology (11th ed.). McGraw-Hill Education. Biorender Transcript Introduction0:06Regulation of the Heartbeat Physiology What’s up, Taim talks med here. Let’s continue our Complete Cheat Code for Heart Physiology.0:13We’re doing this in 4 segments. The 1st video was about the different types of cardiac muscle, the action potentials of pace maker cells and contractile myocardium,0:22and the general properties of our cardiomyocytes. The 2nd video was about the cardiac cycle where we0:28made an easy diagram illustrating what actually happens at each phase. The 3rd video covered0:33everything you need to know regarding the cardiac output. This is the 4th video where we’ll cover the regulation of the
Cardiac Output
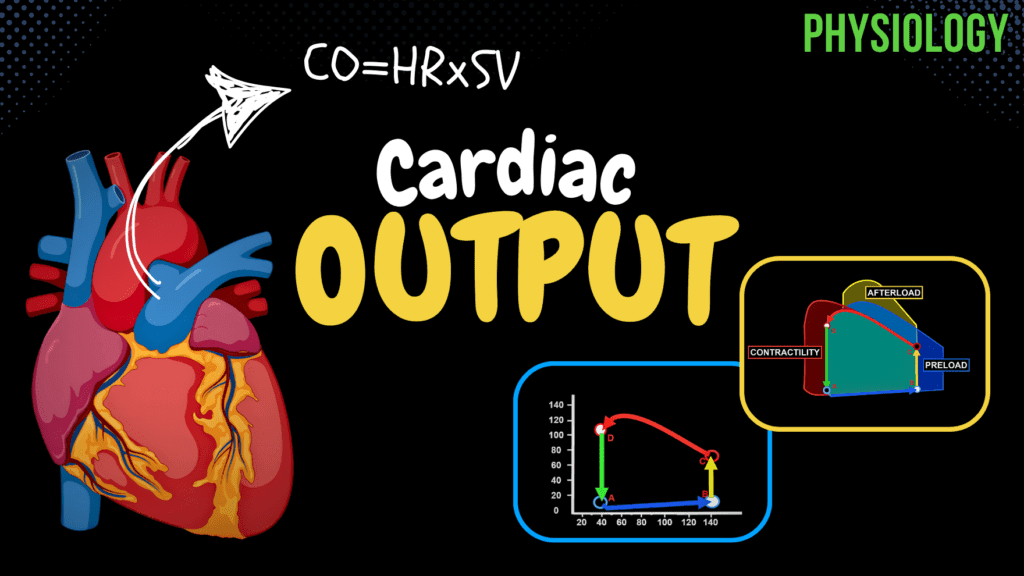
Cardiac Output (Preload, Afterload, Pressure-Volume Diagram) Official Links Instagram Youtube Jki-discord Notes & Illustrations Quizzes Summary & Transcript 📢 Currently, there is no PDF for this video.If you’re interested in having one, feel free to send an inquiry, and I may create it in the future. BUT! There’s a quiz available in the next tab. 12345678910 Cardiac Output – QUIZ Test your understanding with 10 random multiple-choice questions from the question bank. You're in the preview mode. Note: All elements work correctly on the front end. 1 / 10 What is the maximum pressure-volume relationship? A) Constant pressure B) Relationship between pressure and volume C) No relationship D) Sudden increase in pressure The pressure-volume relationship shows the heart’s response to end-diastolic volume and systolic pressure. 2 / 10 What does the ejection fraction measure? A) Amount of blood remaining in ventricles B) Percentage of blood ejected C) Resistance during contraction D) Maximum stroke volume Ejection fraction measures the percentage of blood ejected from the ventricle relative to end-diastolic volume. 3 / 10 What is the approximate stroke volume in a resting adult? A) 100-150 ml B) 50-100 ml C) 30-50 ml D) 10-30 ml Stroke volume is about 50-100 ml per beat. 4 / 10 What is the relationship between stroke volume and cardiac output? A) Independent of heart rate B) Inversely proportional to afterload C) Directly proportional to heart rate D) Directly proportional to cardiac output Stroke volume multiplied by heart rate determines cardiac output. 5 / 10 How does heart rate influence cardiac output at very high rates (>150 bpm)? A) Increases cardiac output B) Has no effect C) Decreases cardiac output D) Causes arrhythmias Cardiac output decreases at very high heart rates due to insufficient ventricular filling. 6 / 10 What is the physiological significance of the pressure-volume loop? A) Assess heart function B) Predict arrhythmias C) Measure blood oxygenation D) Analyze electrical activity Pressure-volume loops help evaluate heart function and valve health. 7 / 10 What is the normal cardiac output at rest? A) 10-12 liters B) 2-3 liters C) 5-7 liters D) 15-20 liters Normal cardiac output at rest is 5-7 liters per minute. 8 / 10 How does contractility affect cardiac output? A) Lowers cardiac reserve B) Reduces ventricular filling C) Enhances cardiac output D) Stabilizes blood pressure Increased contractility leads to stronger ventricular contractions, enhancing cardiac output. 9 / 10 What is the term for the amount of blood in the ventricles before contraction? A) Stroke volume B) Preload C) Contractility D) Afterload Preload refers to the volume of blood in the ventricles before contraction. 10 / 10 What is the approximate cardiac output at rest in a healthy adult? A) 8-10 liters B) 5-7 liters C) 2-3 liters D) 12-15 liters Cardiac output at rest is about 5-7 liters per minute. Your score is The average score is 0% Description Complete Cheat Code for Heart Physiology: 1st Video: Types of cardiac muscle, action potentials of pacemaker cells and contractile myocardium, and general properties of cardiomyocytes. 2nd Video: Detailed exploration of the cardiac cycle, including phase-by-phase events, valve operations, and pressure differences. 3rd Video: Cardiac output. 4th Video: Regulation of heartbeat. What is Cardiac Output? Definition: The amount of blood ejected from each ventricle per minute. Formula: Cardiac Output = Heart Rate (bpm) × Stroke Volume (L/beat) Units: Measured in liters per minute (L/min). Visualizing Cardiac Output Heart Anatomy: Right and left atria, ventricles, aorta. Cardiac Cycle Phases: Atrial systole Isovolumetric contraction Ejection phase (systolic phase) Isovolumetric relaxation Passive filling phase (common diastolic phase) Stroke Volume: Amount of blood ejected per beat (~50-100 ml). Heart Rate: Number of beats per minute. Factors Determining Cardiac Output Heart Rate: Increased HR typically increases cardiac output, but >150 bpm may reduce it due to inadequate ventricular filling. Stroke Volume: Depends on: Venous Return: More blood entering the heart leads to greater output. Contractility: Stronger contractions eject more blood. Aortic Resistance: Higher resistance (hypertension, plaque) reduces stroke volume. Normal Cardiac Output At Rest: ~5-7 L/min During Exercise: ~15-30 L/min Pressure-Volume Relationship Diastolic Phase: Ventricular filling, gradual pressure increase. Systolic Phase: Ventricular contraction, pressure rises then falls. Isovolumetric Phases: Contraction and relaxation phases with no volume change. Clinical Relevance Pressure-Volume Curves: Assess heart function, muscle efficiency, and valve health. Abnormal PV Loops: Right Shift: Increased preload (more blood in, more ejected). Increased Afterload: Higher aortic pressure, harder for the heart to eject blood. Increased Contractility: Stronger contractions, more blood ejected. Factors Affecting Cardiac Output Preload: Volume of blood before contraction. Afterload: Resistance ventricles overcome to eject blood. Contractility: Strength of ventricular contraction. Regulation of Heartbeat Mechanisms: Myogenic, neural, and humoral regulation. Conclusion Summary: Discussed cardiac output, pressure-volume curve, and effects of preload, afterload, and contractility. Next Video: Regulation of heartbeat. #cardiacphysiology #heartfunction #cardiacoutput #ecg #medicaleducation #usmlepreparation #nursingeducation #premed #heartanatomy Sources: University lectures and notes Barrett, K. E., Barman, S. M., Boitano, S., & Brooks, H. L. (2016). Ganong’s Review of Medical Physiology (25th ed.). McGraw-Hill Education. Hall, J. E. (2016). Guyton and Hall Textbook of Medical Physiology (13th ed.). Elsevier. Mohrman, D. E., & Heller, L. J. (2014). Cardiovascular Physiology (11th ed.). McGraw-Hill Education. Biorender Transcript Introduction0:08What’s up, Taim talks med here. Let’s continue our Complete Cheat Code for Heart Physiology.0:13We’re doing this in 4 segments. The 1st video was about the different types of cardiac muscle,0:18the action potentials of pace maker cells and contractile myocardium, and the general0:22properties of our cardiomyocytes. In the 2nd video we looked detailed into the cardiac cycle. In this0:28video we’re gonna cover everything you need to know regarding the cardiac output. And in0:33the next video we’ll cover the regulation of the Heartbeat, covering all the most0:38important mechanisms that actually change the contractility and heart rate. Alright awesome.What is Cardiac Output?0:44Now how do we define cardiac output? Cardiac output is the mount of blood that is ejected0:50from each ventricle during one contraction. Let’s visualize this. Here’s the heart. We got0:56the right and the left atria, the right and the left ventricles, and
Cardiac Cycle
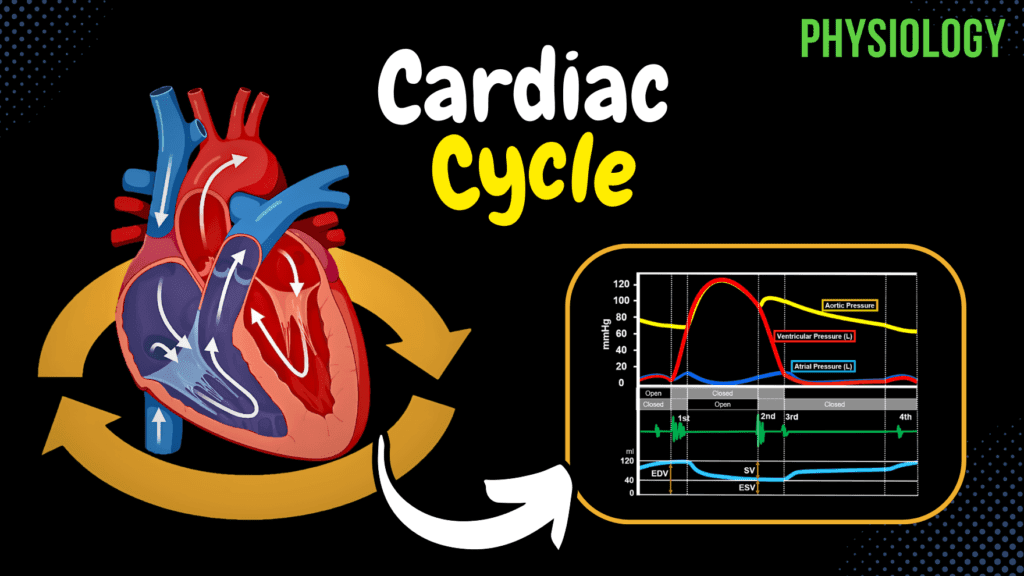
Cardiac Cycle (Pressure-Graph) Official Links Instagram Youtube Jki-discord Notes & Illustrations Quizzes Summary & Transcript 📢 Currently, there is no PDF for this video.If you’re interested in having one, feel free to send an inquiry, and I may create it in the future. BUT! There’s a quiz available in the next tab. 12345678910 Cardiac Cycle – QUIZ Test your understanding with 10 random multiple-choice questions from the question bank. You're in the preview mode. Note: All elements work correctly on the front end. 1 / 10 What does the cardiac cycle refer to? A) Pressure differences in the heart B) Valve mechanics C) Electrical conduction of the heart D) Mechanical events of one heartbeat The cardiac cycle includes the phases of contraction and relaxation during one heartbeat. 2 / 10 What does stroke volume (SV) depend on? A) EDV and ESV B) Ventricular relaxation C) Blood oxygen content D) Atrial pressure SV depends on end-diastolic volume, end-systolic volume, and myocardial contractility. 3 / 10 Which heart sound is most commonly absent in healthy adults? A) S3 B) S1 C) S4 D) S2 S4 is typically absent in healthy adults and indicates strong atrial contraction when present. 4 / 10 Which phase of the cardiac cycle involves no change in blood volume but increased pressure? A) Ventricular ejection B) Isovolumetric contraction C) Passive filling D) Atrial systole Isovolumetric contraction involves increased ventricular pressure without a change in volume. 5 / 10 What is the normal range for the ejection fraction (EF)? A) 40-50% B) 20-40% C) 60-80% D) 50-70% The normal EF range is 50-70%, indicating the percentage of EDV ejected during systole. 6 / 10 What is the primary cause of the second heart sound (S2)? A) Semilunar valve closure B) Blood exiting atria C) AV valve closure D) Blood entering ventricles S2 is caused by the closure of semilunar valves at the start of diastole. 7 / 10 Which phase of the cardiac cycle involves atrial contraction? A) Isovolumetric contraction B) Ventricular ejection C) Atrial systole D) Passive filling Atrial systole is the phase where both atria contract to push blood into the ventricles. 8 / 10 What heart sound is heard during the closure of AV valves? A) S2 B) S3 C) S1 D) S4 The first heart sound (S1) occurs during AV valve closure at the start of ventricular systole. 9 / 10 Which phase is characterized by the AV valves opening and blood entering the ventricles? A) Passive filling B) Isovolumetric contraction C) Atrial systole D) Isovolumetric relaxation Passive filling is characterized by AV valve opening and blood flow into the ventricles. 10 / 10 Which heart sound corresponds to semilunar valve closure? A) S4 B) S3 C) S1 D) S2 The second heart sound (S2) is heard during the closure of the semilunar valves. Your score is The average score is 0% Description Complete Cheat Code for Heart Physiology Series: 1st Video: Types of cardiac muscle, action potentials of pacemaker cells and contractile myocardium, and general properties of cardiomyocytes. 2nd Video: Detailed exploration of the cardiac cycle, including phase-by-phase events, valve operations, and pressure differences. 3rd Video: Cardiac output. 4th Video: Regulation of heartbeat. Phases of the Cardiac Cycle: The cardiac cycle consists of mechanical events in one heartbeat, including contraction (systole) and relaxation (diastole). Atrial Systole (0.1s): Atria contract, pushing blood into ventricles. Isovolumetric Contraction (0.04s): Ventricles contract, but valves remain closed. Ventricular Ejection (0.26s): Ventricles push blood into the aorta and pulmonary artery. Isovolumetric Relaxation (0.08s): Ventricles relax, no blood flow into ventricles. Passive Filling (0.32s): AV valves open, ventricles fill passively. Valve Operations and Pressure Differences: Bottle Cap Phenomenon: Demonstrates how pressure controls valve function. Pressure Curve and Graphical Representation: Vertical Axis: Blood pressure (mmHg). Horizontal Axis: Time (seconds). Red: Left ventricular pressure. Blue: Left atrial pressure. Yellow: Aortic pressure. Heart Sounds: S1 (First Heart Sound): Closure of AV valves, start of systole. S2 (Second Heart Sound): Closure of semilunar valves, start of diastole. S3 (Third Heart Sound): Passive ventricular filling. S4 (Fourth Heart Sound): Strong atrial contraction. Ventricular Volumes: End Diastolic Volume (EDV): 110-150 ml. Stroke Volume (SV): 60-100 ml. Reserve Volume: 20-40 ml. Residual Volume: Volume never ejected. Ejection Fraction (EF): Normal 50-70%, reduced in heart failure. #cardiacphysiology #heartfunction #cardiaccycle #ecg #medicaleducation #usmlepreparation #nursingeducation #premed #heartanatomy Sources: University lectures and notes. Barrett, K. E., Barman, S. M., Boitano, S., & Brooks, H. L. (2016). Ganong’s Review of Medical Physiology (25th ed.). McGraw-Hill Education. Hall, J. E. (2016). Guyton and Hall Textbook of Medical Physiology (13th ed.). Elsevier. Mohrman, D. E., & Heller, L. J. (2014). Cardiovascular Physiology (11th ed.). McGraw-Hill Education. Biorender. Transcript Introduction0:08What s up, Taim talks med here. Let s continue our Complete Cheat Code for Heart Physiology.0:13We re doing this in 4 segments. The 1st video was about the different types of cardiac muscle,0:18the action potentials of pace maker cells and contractile myocardium, and the general0:22properties of our cardiomyocytes. In this video we will look detailed into the cardiac cycle,0:28and draw a curve and understand what happens at each phase. In the 3rd video we ll cover0:33everything you need to know regarding the cardiac output. And in the 4th video where we ll cover0:38the regulation of the Heartbeat, covering all the most important mechanisms that actually change the0:43contractility and heart rate. Alright awesome. Cardiac cycle is basically just the beginningWhat is Cardiac Cycle?0:50of one heartbeat to the beginning of the next. And it includes all the mechanical0:55events happening within one heartbeat. So If you look here, this is the heart,1:00and here it s pumping continuously. Showing you one cardiac cycle after the other,1:05and if we remove the walls as it s pumping, you ll see that there are specific events happening.1:11And if you just stare at this heart, focus on one chamber, you ll notice that one cardiac1:17cycle consists of two periods: one during which the heart muscle relaxes and refills with blood,1:23called diastole, following a period of contraction and pumping of blood, called systole.1:29What we
Cardiac Muscle
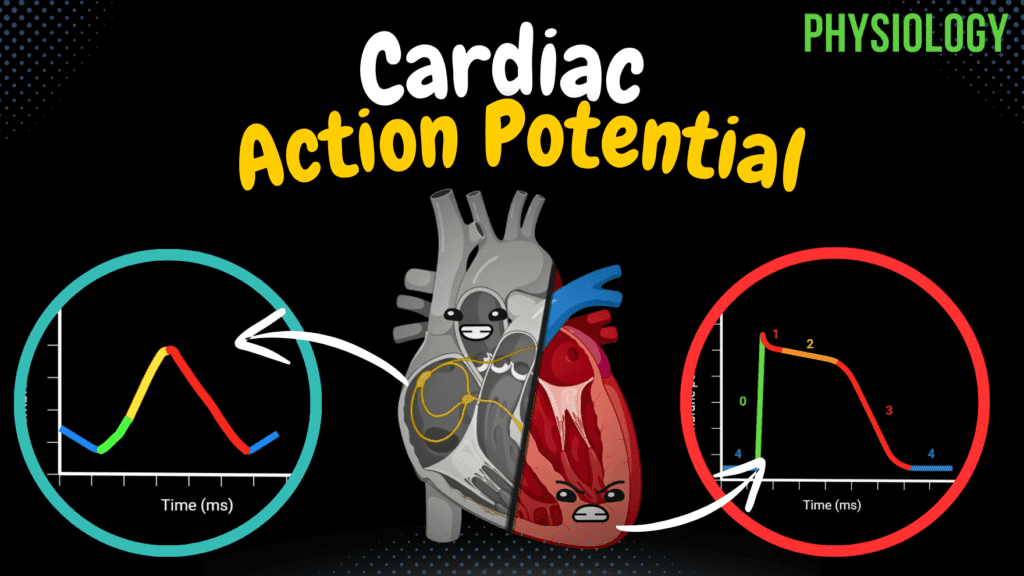
Cardiac Muscle (Action Potential, Automaticity, ARP, RRP) Official Links Instagram Youtube Jki-discord Notes & Illustrations Quizzes Summary & Transcript 📢 Currently, there is no PDF for this video.If you’re interested in having one, feel free to send an inquiry, and I may create it in the future. BUT! There’s a quiz available in the next tab. 12345678910 Cardiac Muscle – QUIZ Test your understanding with 10 random multiple-choice questions from the question bank. You're in the preview mode. Note: All elements work correctly on the front end. 1 / 10 What is the function of atrial natriuretic peptide (ANP)? A) Increases heart rate B) Stimulates vasoconstriction C) Promotes vasodilation D) Contracts the myocardium ANP promotes vasodilation and reduces sodium and water reabsorption in the kidneys to regulate blood volume. 2 / 10 What is the stable resting membrane potential of contractile cells? A) -60 mV B) -85 mV C) 0 mV D) -90 mV Contractile cells have a stable resting membrane potential of approximately -85 mV. 3 / 10 What is the primary pacemaker of the heart? A) SA node B) Purkinje fibers C) AV node D) Bundle of His The sinoatrial (SA) node is the primary pacemaker of the heart, setting the rhythm at 60-80 beats per minute. 4 / 10 What is the primary function of pacemaker cells in the heart? A) Promote vasodilation B) Secrete hormones C) Generate and propagate electrical impulses D) Contract the myocardium Pacemaker cells generate and propagate electrical impulses due to their automaticity. 5 / 10 Which ion is responsible for the rapid depolarization (Phase 0) of contractile cells? A) Cl- B) Ca2+ C) Na+ D) K+ Na+ influx through voltage-gated sodium channels causes rapid depolarization in contractile cells. 6 / 10 What structure sets the primary rhythm of the heart? A) Bundle of His B) SA node C) AV node D) Purkinje fibers The sinoatrial (SA) node is the heart’s primary pacemaker. 7 / 10 What is the primary location of contractile cardiomyocytes? A) Endocardium B) SA node C) Myocardium D) Epicardium Contractile cardiomyocytes are located in the myocardium. 8 / 10 Why does the AV node delay conduction of electrical impulses? A) To speed up conduction B) To stabilize action potentials C) To synchronize heart sounds D) To allow atrial contraction The AV node slows conduction (0.1 m/s) to ensure atrial contraction before ventricular contraction. 9 / 10 What ion influx is critical during the plateau phase of contractile cells? A) K+ B) Ca2+ C) Cl- D) Na+ Ca2+ influx through L-type channels is critical during the plateau phase. 10 / 10 Which layer of the heart generates the contraction force? A) Epicardium B) Endocardium C) Pericardium D) Myocardium The myocardium is responsible for generating the heart’s contractile force. Your score is The average score is 0% Description Complete Cheat Code for Heart Physiology Series: 1st Video: Types of cardiac muscle, action potentials of pacemaker cells and contractile myocardium, and general properties of cardiomyocytes. 2nd Video: Detailed exploration of the cardiac cycle, including phase-by-phase events, valve operations, and pressure differences. 3rd Video: Cardiac output. 4th Video: Regulation of heartbeat. Types of Cardiac Muscle Cells: 1. Pacemaker Cells (Nodal Cells): Location: SA node, AV node, Bundle of His, RBB, LBB, Purkinje fibers. Function: Generate and propagate electrical impulses. Action Potential: No stable resting membrane potential. “Funny” Na+ channels allow slow Na+ influx, triggering depolarization. T-type and L-type Ca2+ channels open, causing a rapid influx of Ca2+. Repolarization occurs via K+ efflux. 2. Contractile Cells: Location: Myocardium. Function: Generate the force of contraction. Action Potential: Stable resting membrane potential (-85 mV). Depolarization via Na+ influx, plateau phase due to Ca2+ influx balanced by K+ efflux, followed by repolarization. 3. Endocrine Cells: Location: Atria and ventricles. Function: Secrete ANP and BNP to regulate blood pressure and fluid balance. Conduction System of the Heart: SA Node: Primary pacemaker (60-80 BPM). AV Node: Secondary pacemaker (40-60 BPM), slows conduction. Bundle of His and Purkinje Fibers: Rapidly conduct impulses through ventricles. Action Potentials: A Comparative View Pacemaker Cells: Phase 4: Slow depolarization via “funny” Na+ channels. Phase 0: Rapid depolarization via Ca2+ influx. Phase 3: Repolarization via K+ efflux. Contractile Cells: Phase 0: Rapid depolarization via Na+ influx. Phase 1: Initial repolarization via K+ efflux. Phase 2: Plateau phase via Ca2+ influx. Phase 3: Repolarization via K+ efflux. Phase 4: Resting membrane potential. Electrical Conduction Pathway: Impulse generation at SA Node. Atrial conduction (1 m/s). AV Node delay (0.1 m/s) ensures proper atrial emptying. Ventricular conduction via Purkinje fibers (1-4 m/s). Refractory Periods: Absolute Refractory Period (ARP): No response to stimuli. Relative Refractory Period (RRP): Strong stimulus may trigger an action potential. Effective Refractory Period (ERP): Combination of ARP and early RRP. Properties of Cardiomyocytes: Automaticity All-or-none law Long refractory periods Sources: University lectures and notes Barrett, K. E., Barman, S. M., Boitano, S., & Brooks, H. L. (2016). Ganong’s Review of Medical Physiology (25th ed.). McGraw-Hill Education. Hall, J. E. (2016). Guyton and Hall Textbook of Medical Physiology (13th ed.). Elsevier. Mohrman, D. E., & Heller, L. J. (2014). Cardiovascular Physiology (11th ed.). McGraw-Hill Education. Biorender Transcript Introduction0:08What s up, Taim talks med here. I ve now simplified all the most important high yield topics in heart physiology, so this is the Complete Cheat Code0:18We re doing this in 4 segments. This is the 1st video where we re going talk detailed about the different types of cardiac muscle, the action potentials of pace maker cells and contractile0:27myocardium, and the general properties of our cardiomyocytes. The 2nd video will be about the cardiac cycle. The 3rd video we ll cover everything you need to know regarding the0:36cardiac output. And in the 4th video we ll cover the regulation of the Heartbeat, covering all the0:42most important mechanisms that actually change the contractility and heart rate. Alright awesome.You should already know0:48Alright, so I m starting this video assuming that you have some pre knowledge in the anatomy of the0:54heart. I m basically assuming that you already know