
Knee Joint Anatomy & Common Injuries (Ligaments, Menisci & Movements)
Knee Joint Anatomy & Common Injuries (Ligaments, Menisci & Movements) Official Links Instagram Youtube Jki-discord Notes & Illustrations Quizzes Summary & Transcript The PDF for this topic is not available yetIt’s expected to be published by December 2025.In the meantime, test your knowledge using the QUIZ under the next tab! 12345678910 Knee Joint Test your understanding with 10 random multiple-choice questions from the question bank. You're in the preview mode. Note: All elements work correctly on the front end. 1 / 10 Which structure lies between the skin and patella? A) Patellar ligament B) Infrapatellar fat pad C) Subcutaneous prepatellar bursa D) Medial meniscus The subcutaneous prepatellar bursa cushions the front of the patella. 2 / 10 Which ligament reinforces the posterior‑lateral capsule? A) Oblique popliteal ligament B) Tibial collateral ligament C) Fibular collateral ligament D) Arcuate popliteal ligament The arcuate popliteal ligament supports posterolateral reinforcement. 3 / 10 Which ligament connects the lateral meniscus to the medial femoral condyle? A) Posterior meniscofemoral ligament B) Meniscotibial ligament C) Transverse ligament D) Anterior meniscofemoral ligament The anterior meniscofemoral ligament does this. 4 / 10 Which structures deepen the tibial plateau and absorb shock? A) Retinacula B) Bursae C) Menisci D) Ligaments The menisci enhance congruency and reduce impact. 5 / 10 Which ligament is a continuation of the quadriceps tendon? A) Oblique popliteal ligament B) ACL C) PCL D) Patellar ligament The patellar ligament continues from the quadriceps tendon. 6 / 10 Which structure connects medial femoral condyle to tibia? A) PCL B) Tibial collateral ligament C) ACL D) Fibular collateral ligament The tibial collateral ligament connects those two structures. 7 / 10 Which ligament connects the apex of the patella to the tibial tuberosity? A) Patellar ligament B) Tibial collateral ligament C) Quadriceps tendon D) Fibular collateral ligament The patellar ligament links the patella to the tibial tuberosity. 8 / 10 What is the shape of the medial meniscus? A) Semicircular B) O-shaped C) C-shaped D) Rounded The medial meniscus is C-shaped and less mobile. 9 / 10 Which bones articulate at the femorotibial joint? A) Proximal femur and tibia B) Distal femur and proximal tibia C) Distal femur and fibula D) Proximal tibia and fibula The distal femur condyles articulate with the proximal tibia. 10 / 10 Which ligament prevents posterior tibial displacement? A) ACL B) PCL C) Fibular collateral ligament D) Tibial collateral ligament The PCL stops backward sliding of the tibia. Your score is The average score is 0% Description This video covers the full anatomy of the knee joint, followed by a breakdown of common injuries like ACL tear, meniscus tear, osteoarthritis, and bursitis. Bones of the Knee Joint Femur (femur): Forms the upper part of the knee joint.Tibia (tibia): Bears weight and forms the lower part of the joint.Patella (patella): Protects the anterior surface and improves leverage of the quadriceps. Articulations Femorotibial joint: Between femoral condyles and tibial plateau.Femoropatellar joint: Between femur and posterior patella. Menisci of the Knee Medial meniscus (meniscus medialis): C-shaped; less mobile; firmly attached to tibia.Lateral meniscus (meniscus lateralis): Nearly circular; more mobile. Intra-articular Ligaments Meniscotibial ligaments (ligg. meniscotibialia)Transverse ligament of the knee (ligamentum transversum genus)Anterior meniscofemoral ligament (Humphrey) (ligamentum meniscofemorale anterius)Posterior meniscofemoral ligament (Wrisberg) (ligamentum meniscofemorale posterius)Anterior cruciate ligament (ACL) (ligamentum cruciatum anterius): Prevents anterior tibial displacement.Posterior cruciate ligament (PCL) (ligamentum cruciatum posterius): Prevents posterior tibial displacement. Joint Capsule Synovial membrane (membrana synovialis): Produces synovial fluid for lubrication.Fibrous membrane (membrana fibrosa): Outer supportive layer. Extracapsular Ligaments & Retinacula Medial patellar retinaculum: Fibrous expansion supporting the patella.Lateral patellar retinaculum: Stabilizes the patella laterally.Medial patellofemoral ligament: Anchors patella to medial femur.Lateral patellofemoral ligament: Anchors patella to lateral femur.Patellar ligament (ligamentum patellae): Connects patella to tibial tuberosity.Oblique popliteal ligament (ligamentum popliteum obliquum): Reinforces posterior capsule.Arcuate popliteal ligament (ligamentum popliteum arcuatum): Posterolateral reinforcement.Tibial collateral ligament (ligamentum collaterale tibiale): Resists valgus stress.Fibular collateral ligament (ligamentum collaterale fibulare): Resists varus stress.Anterolateral ligament Fat Pads: Infrapatellar fat pad (corpus adiposum infrapatellare): Cushions anterior joint space. Bursae Around the Knee Subcutaneous prepatellar bursa (bursa prepatellaris subcutanea): Over patella; prone to swelling.Subcutaneous infrapatellar bursa (bursa infrapatellaris subcutaneaDeep infrapatellar bursa (bursa infrapatellaris profunda)Suprapatellar bursa (bursa suprapatellaris)Anserine bursa (bursa anserina)Subtendinous bursa of gastrocnemius (bursa subtendinea m. gastrocnemii)Semimembranosus bursa (bursa m. semimembranosi) Movements of the Knee Flexion (flexio): Bending the knee backward.Extension (extensio): Straightening the leg forward.Internal rotation (rotatio interna)External rotation (rotatio externa) Common Knee Joint Conditions Osteoarthritis Progressive degeneration of articular cartilage leading to joint space narrowing and osteophyte formation.Common in older adults, especially women, and those with obesity or previous injuries.Symptoms: joint pain, morning stiffness under 30 mins, crepitus, swelling, reduced range of motion. Meniscus Tear Common in athletes, often due to twisting injuries with a fixed foot.Peripheral tears (in outer vascular zone) may heal conservatively.Symptoms: localized joint pain, delayed swelling, stiffness, difficulty squatting. ACL Tear Often occurs with pivoting, sudden stops, or awkward landings.Common in female athletes.Symptoms: audible pop, rapid swelling, instability, limited motion. Prepatellar Bursitis Inflammation of the bursa in front of the patella.Caused by repeated kneeling, direct trauma, or infection.Symptoms: anterior swelling, pain with pressure or movement, redness, possible fever. Sources Kozlowski, T. (2017). Memorix Anatomy, 2nd ed.Standring, S. (2020). Gray’s Anatomy, 42nd editionWhite TD, Folkens PA. (2005). The Human Bone ManualTubbs RS, Shoja MM, Loukas M. (2016). Bergman’s Encyclopedia of Human Anatomic VariationMoore, K.L., Dalley, A.F., Agur, A.M.R. Clinically Oriented AnatomyKenhub.com Tools Used: Complete Anatomy (3D4Medical), PowerPoint, Canva, Camtasia Transcript 0:00:00.080,0:00:04.720The knee joint is the largest and one of themost complex joints in the body. It carries 0:00:04.720,0:00:10.400our entire weight and that’s exactly whyit’s so prone to problems, meniscal tears, 0:00:10.400,0:00:15.920ligament injuries, patellar dislocations, and ofcourse, wear and tear like osteoarthritis show 0:00:15.920,0:00:21.520up in clinics all the time. But to understand whythese things happen, we need to go inside the knee 0:00:21.520,0:00:26.560joint—look at how it’s built from the inside out.So in this video, we’re going to break down the 0:00:26.560,0:00:31.280full anatomy of the knee joint: the menisci,its capsule, the ligaments, the patella, 0:00:31.280,0:00:36.160the bursae and how it all comes together inmovement. And as always, I’ll
Hip Joint Anatomy & Common Injuries (Ligaments, Capsule, Movement)
Hip Joint Anatomy & Common Injuries (Ligaments, Capsule, Movement) Official Links Instagram Youtube Jki-discord Notes & Illustrations Quizzes Summary & Transcript The PDF for this topic is not available yetIt’s expected to be published by December 2025.In the meantime, test your knowledge using the QUIZ under the next tab! 12345678910 Hip Joint Test your understanding with 10 random multiple-choice questions from the question bank. You're in the preview mode. Note: All elements work correctly on the front end. 1 / 10 What sensation often accompanies hip osteoarthritis? A) Sharp shooting pain B) Cooling sensation C) Crepitus D) Numbness Crepitus is a grating sensation from cartilage wear. 2 / 10 What region articulates with the femoral head? A) Acetabular notch B) Lunate surface C) Acetabular fossa D) Pulvinar acetabuli The lunate surface of the acetabulum is the cartilage-lined articular area. 3 / 10 Which cartilage covers the femoral head? A) Fibrocartilage B) Hyaline cartilage C) Elastic cartilage D) Perichondrium Hyaline cartilage ensures smooth articulation. 4 / 10 Where does the pubofemoral ligament attach? A) Pubis to intertrochanteric line B) Pubis to femoral neck C) Ilium to femur head D) Ischium to greater trochanter Attaches pubic acetabulum to femoral neck. 5 / 10 What drug can raise uric acid and trigger gout? A) Insulin B) Thiazide diuretics C) NSAIDs D) Statins Thiazide diuretics reduce uric acid excretion. 6 / 10 Which hip disease causes symmetrical joint destruction and pannus formation? A) Gout B) Osteoarthritis C) Rheumatoid arthritis D) Avascular necrosis Rheumatoid arthritis is autoimmune and symmetric. 7 / 10 Which ligament bridges the acetabular notch beneath the femoral head? A) Iliofemoral ligament B) Ligament of head of femur C) Transverse acetabular ligament D) Pubofemoral ligament The transverse acetabular ligament connects across the notch. 8 / 10 What type of joint is the hip joint? A) Hinge joint B) Saddle joint C) Pivot joint D) Ball-and-socket joint The hip is a ball-and-socket synovial joint allowing multi-directional movement. 9 / 10 What dietary factor worsens gout risk? A) High-purine diet B) High sugar diet C) High calcium diet D) High fiber diet High-purine foods like red meat and beer increase uric acid. 10 / 10 Which demographic is most commonly affected by hip osteoarthritis? A) Men 30‑50 B) Elderly >60 C) Female teens D) Premenopausal women Elderly adults over 60 due to wear‑and‑tear. Your score is The average score is 0% Description This video is about the Hip Joint.In this video, we break down the anatomy of the hip joint, how it moves, what supports it, and what happens when it gets damaged. We go layer by layer, starting with the bones and landmarks of the acetabulum and femur, then look at the joint capsule, synovial membrane, ligaments, and finish off by exploring three common conditions that affect the hip joint: osteoarthritis, gout, and rheumatoid arthritis.________________________________________Structures of the Hip JointBony structures involved• Head of femur (caput femoris): Articulates with the acetabulum to form the ball-and-socket joint.• Acetabulum (acetabulum): Concave socket in the pelvis that receives the head of the femur.Acetabular landmarks• Acetabular margin (margo acetabuli): The rim surrounding the acetabulum.• Acetabular notch (incisura acetabuli): A gap in the inferior rim of the acetabulum.• Lunate surface (facies lunata): Smooth, crescent-shaped surface that contacts the femoral head.• Acetabular fossa (fossa acetabuli): Central, non-articular depression in the acetabulum. Intra-articular structures• Acetabular labrum (labrum acetabulare): Fibrocartilaginous rim that deepens the socket and improves joint stability.• Transverse acetabular ligament (ligamentum transversum acetabuli): Bridges the acetabular notch to complete the socket rim.• Ligament of the head of femur (ligamentum capitis femoris): Connects the fovea of femoral head to the acetabular fossa and carries a small artery.• Acetabular fat pad (pulvinar acetabuli): Fat within the acetabular fossa that cushions and supports the ligament.Joint capsule• Synovial membrane (membrana synovialis): Inner layer of capsule producing synovial fluid.• Fibrous membrane (membrana fibrosa): Outer dense connective tissue layer providing mechanical stability.Capsular ligaments• Iliofemoral ligament (ligamentum iliofemorale): Y-shaped ligament from anterior inferior iliac spine to intertrochanteric line; resists hyperextension.• Pubofemoral ligament (ligamentum pubofemorale): Extends from pubic part of acetabulum to lower femoral neck; resists abduction and extension.• Ischiofemoral ligament (ligamentum ischiofemorale): Spirals from ischium to posterior femur; limits internal rotation.________________________________________Hip Joint Movements• Flexion (flexio): Thigh moves forward.• Extension (extensio): Thigh moves backward.• Abduction (abductio): Thigh moves laterally away from body.• Adduction (adductio): Thigh moves medially toward body.• Internal rotation (rotatio interna): Femur rotates inward.• External rotation (rotatio externa): Femur rotates outward.________________________________________Common Conditions Affecting the Hip JointOsteoarthritis (OA) Pathophysiology• Degeneration of articular cartilage leads to joint space narrowing.• Bone-on-bone friction causes inflammation and osteophyte (bone spur) formation.• Risk factors: age, obesity, physical labor, joint trauma.• Symptoms: groin pain, stiffness less than 30 mins in the morning, reduced range of motion, crepitus.Gout Pathophysiology• Deposition of monosodium urate crystals in synovial membrane.• Causes acute inflammatory arthritis (synovitis).• Risk factors: CKD, obesity, purine-rich diet, alcohol, thiazide diuretics.• Symptoms: sudden pain, swelling, warmth, redness, extreme tenderness.Rheumatoid Arthritis (RA) Pathophysiology• Autoimmune disease targeting the synovial membrane.• Leads to pannus formation and joint destruction.• Risk factors: female sex, age 40–60, HLA-DR4, smoking.• Symptoms: symmetrical joint pain, stiffness longer than 30 mins, fatigue, deformity.________________________________________If you want a PDF version of this lecture, test your knowledge with a quiz, or explore a structured list of all anatomy videos, visit my website: taimtalksmed.com Sources:• Kozlowski, T. (2017). Memorix Anatomy, 2nd ed.• Standring, S. (2020). Gray’s Anatomy, 42nd edition• Tubbs RS, Shoja MM, Loukas M. (2016). Bergman’s Encyclopedia of Human Anatomic Variation• White TD, Folkens PA. (2005). The Human Bone Manual• Moore, K.L., Dalley, A.F., & Agur, A.M.R. (Clinically Oriented Anatomy)• Kenhub.com• Medscape Programs used: Complete Anatomy (3D4Medical), PowerPoint, Canva, Camtasia Summary written by ChatGPT Transcript 0:00:00.080,0:00:04.320As we get older, one of the most commonproblems we run into is that our joints 0:00:04.320,0:00:08.800start to wear down. And one that canoften get inflamed – is the hip joint. 0:00:08.800,0:00:13.360Some people feel stiffness in the morning,others feel pain after a long walk. 0:00:13.360,0:00:19.200But to understand why, we need to go inside thehip joint, look at how it’s built
Wrist & Hand Joints (Radiocarpal, Intercarpal, CMC, MCP & IP) | Anatomy
Wrist & Hand Bones (Carpals, Metacarpals & Phalanges) | Anatomy Official Links Instagram Youtube Jki-discord Notes & Illustrations Quizzes Summary & Transcript The PDF for this topic is not available yetIt’s expected to be published by December 2025.In the meantime, test your knowledge using the QUIZ under the next tab! 12345678910 Hand Joints Test your understanding with 10 random multiple-choice questions from the question bank. You're in the preview mode. Note: All elements work correctly on the front end. 1 / 10 What joint lies between the proximal and distal rows of carpal bones? A) Carpometacarpal joint B) Intermetacarpal joint C) Radiocarpal joint D) Midcarpal joint The midcarpal joint connects the two rows of carpals. 2 / 10 Which joint allows thumb opposition? A) CMC joint of index finger B) Intermetacarpal joint C) MCP joint of thumb D) Saddle CMC joint of thumb The first carpometacarpal (CMC) joint is a saddle joint permitting opposition. 3 / 10 How many CMC joints connect the carpus to the palm? A) Five B) Six C) Four D) Three There are five CMC joints, one for each metacarpal base. 4 / 10 What ligaments reinforce MCP joints? A) Annular ligaments B) Collateral + palmar + deep transverse ligaments C) Collateral ligaments only D) Ligaments of wrist They are supported by collateral, palmar, and deep transverse metacarpal ligaments. 5 / 10 Which joint type describes the interphalangeal joints? A) Pivot B) Ellipsoid C) Ball-and-socket D) Hinge joint IP joints are hinge joints, allowing flexion and extension only. 6 / 10 Which ligament links adjacent metacarpals at their heads? A) Deep transverse metacarpal ligament B) Interosseous membrane C) Palmar aponeurosis D) Dorsal intercarpal ligament The deep transverse metacarpal ligament binds metacarpal heads together. 7 / 10 Which ligaments form the volar plates at PIP and DIP joints? A) Radiocarpal plates B) Volar plates C) MCP plates D) Collateral plates Palmar ligaments (volar plates) resist hyperextension at the interphalangeal joints. 8 / 10 Which ligament resists radial deviation? A) Ulnar collateral ligament B) Palmar radiocarpal ligament C) Dorsal radiocarpal ligament D) Radial collateral ligament The ulnar collateral ligament prevents excessive radial deviation. 9 / 10 Which bones articulate at the radiocarpal (wrist) joint? A) Ulna, triquetrum, lunate B) Radius, articular disc, scaphoid, lunate, triquetrum C) Radius, pisiform, capitate D) Radius, ulna, trapezium The radiocarpal joint is formed by the radius, articular disc, and scaphoid/lunate/triquetrum. 10 / 10 What role do the palmar intercarpal ligaments serve? A) Connect carpal bones palmar side B) Carpal tunnel support C) Wrist flexion D) MCP stability They connect carpal bones and support the wrist’s palmar side. Your score is The average score is 0% Description This video is about the joints of the wrist and hand. In this video I break down every major articulation from the wrist to the fingertips – their anatomy, movement, and supporting ligaments. Radiocarpal joint (Articulatio radiocarpea)• Formed by the carpal articular surface of the radius and the articular disc (part of the triangular fibrocartilage complex)• Articulates with: Scaphoid (os scaphoideum), Lunate (os lunatum), and Triquetrum (os triquetrum)• Type: Ellipsoid (biaxial) joint• Movements: Flexion (palmar flexion), extension (dorsiflexion), abduction (radial deviation), adduction (ulnar deviation)• Ligaments: – Palmar radiocarpal ligament – Palmar ulnocarpal ligament – Dorsal radiocarpal ligament – Dorsal ulnocarpal ligament – Radial collateral ligament – Ulnar collateral ligament• Capsule: Fibrous capsule reinforced by synovial membrane Intercarpal joints (Articulationes intercarpeae)• Between neighboring carpal bones in each row• Type: Plane joints• Ligaments: – Palmar intercarpal ligaments – Dorsal intercarpal ligaments – Interosseous intercarpal ligaments• Function: Stabilize the carpal arch and assist in force transmission during load-bearing tasks Midcarpal joint (Articulatio mediocarpea)• Located between the proximal row and distal row of carpal bones• Not a single joint cavity; rather, a composite joint with an S-shaped contour• Movements: Augments wrist extension and radial/ulnar deviation• Ligaments: Shares palmar and dorsal intercarpal ligaments with adjacent joints Carpometacarpal joints (Articulationes carpometacarpeae)• Between distal carpal row and bases of metacarpals (ossa metacarpi)• Joints of digits II–V: Plane joints with limited motion• Thumb (CMC I): – Saddle joint – Movements: Flexion, extension, abduction, adduction, opposition• Ligaments: – Palmar and dorsal carpometacarpal ligaments Intermetacarpal joints (Articulationes intermetacarpeae)• Between bases of metacarpals II–V• Ligaments: – Dorsal metacarpal ligaments – Palmar metacarpal ligaments – Interosseous metacarpal ligaments• Function: Stabilize hand posture and allow slight gliding Metacarpophalangeal joints (Articulationes metacarpophalangeae)• Between heads of metacarpals and bases of proximal phalanges (phalanges proximales)• Type: Condyloid joints (biaxial)• Movements: Flexion, extension, abduction, adduction, circumduction• Ligaments: – Medial and lateral collateral ligaments – Palmar ligaments (volar plates) – Deep transverse metacarpal ligament Interphalangeal joints (Articulationes interphalangeae)• Digits II–V: – Proximal interphalangeal joint (PIP) – Distal interphalangeal joint (DIP)• Thumb: – One interphalangeal joint only• Type: Hinge joints (uniaxial)• Ligaments: – Medial and lateral collateral ligaments – Palmar ligaments (volar plates)• Function: Allow flexion and extension with strong lateral support Additional ligamentous and fascial structures (not primary joint stabilizers):• Palmar aponeurosis – Protects flexor tendons and stabilizes soft tissue during grip• Superficial transverse metacarpal ligament – Located at distal edge of palmar aponeurosis• Palmar carpal ligament – Forms superficial component of the flexor retinaculum Clinical notes covered:• TFCC injury• Thumb CMC osteoarthritis• Ligament sprains and dislocations• PIP joint instability and hyperextension• Volar plate injury• MCP collateral ligament rupture (Gamekeeper’s thumb)• Joint movement during grasp, grip, and fine motor control Sources:• Kozlowski, T. (2017). Memorix Anatomy, 2nd ed.• Standring, S. (2020). Gray’s Anatomy, 42nd ed.• Platzer, W. (2004). Color Atlas of Human Anatomy Vol. 1: Locomotor System• White TD, Folkens PA. (2005). The Human Bone Manual Programs used: Complete Anatomy, Powerpoint, Canva, Camtasia Transcript 0:00:00.080,0:00:04.480In the last video, we looked at all the bonesin the wrist and hand, but bones on their own 0:00:04.480,0:00:08.880would just fall apart. So how do they stayconnected and move with such control when 0:00:08.880,0:00:13.760you make a fist or flex your fingers?It all comes down to this – the joints. 0:00:13.760,0:00:18.800In this video, we’re going to go through everymajor joint in the wrist and hand. So we will 0:00:18.800,0:00:24.640cover the radiocarpal joint, intercarpal joints,and the midcarpal joint. Then we will move on to 0:00:24.640,0:00:29.760the carpometacarpal joints, intermetacarpaljoints, metacarpophalangeal joints, 0:00:29.760,0:00:33.680and finally, the interphalangeal
Elbow Joint: Ligaments, Movements & Injuries | Clinical Anatomy
Elbow Joint: Ligaments, Movements & Injuries | Clinical Anatomy Official Links Instagram Youtube Jki-discord Notes & Illustrations Quizzes Summary & Transcript The PDF for this topic is not available yetIt’s expected to be published by December 2025.In the meantime, test your knowledge using the QUIZ under the next tab! 12345678910 Elbow Joint Test your understanding with 10 random multiple-choice questions from the question bank. You're in the preview mode. Note: All elements work correctly on the front end. 1 / 10 What injury results from pulling a young child’s arm, displacing the radial head? A) Nursemaid’s elbow B) Tennis elbow C) Golfer’s elbow D) Olecranon bursitis Nursemaid’s elbow is a common subluxation of the radial head. 2 / 10 What type of joint is the humeroulnar articulation? A) Ball-and-socket joint B) Hinge joint C) Gliding joint D) Pivot joint It is a classic hinge joint. 3 / 10 Which joint allows the radius to rotate over the ulna? A) Annular joint B) Humeroulnar joint C) Proximal humeroradial joint D) Proximal radioulnar joint Rotation occurs at the proximal radioulnar joint. 4 / 10 Which deeper bursa lies under the triceps tendon? A) Subtendinous triceps bursa B) Subcutaneous olecranon bursa C) Deltoid bursa D) Bicipital bursa The subtendinous bursa of triceps brachii lies near its insertion. 5 / 10 Which ligament reinforces the lateral side of the elbow capsule? A) Radial collateral ligament B) Ulnar collateral ligament C) Quadrate ligament D) Transverse ligament The radial collateral ligament blends with the annular ligament laterally. 6 / 10 What does the radial collateral ligament blend with? A) Ulnar collateral ligament B) Annular ligament C) Quadrate ligament D) Joint capsule It blends with the annular ligament. 7 / 10 Which articulation permits pronation and supination of the forearm? A) Humeroradial joint B) Proximal radioulnar joint C) Humeroulnar joint D) Capitellar joint The proximal radioulnar joint allows rotational movement of the radius. 8 / 10 Where does the fibrous layer of the elbow capsule attach on the humerus? A) To the deltoid tuberosity B) Just below the epicondyles C) To the glenoid cavity D) To the radial groove It attaches just below the medial and lateral epicondyles. 9 / 10 Which activity can lead to olecranon bursitis? A) Overhead lifting B) Throwing sports C) Leaning on elbows D) Pulling objects Repetitive leaning on elbows causes this condition. 10 / 10 What condition presents with swelling and tenderness over the elbow tip? A) Olecranon bursitis B) Tennis elbow C) Golfer’s elbow D) Biceps tendinopathy Olecranon bursitis is inflammation of the olecranon bursa. Your score is The average score is 0% Description Elbow Joint (Ligaments, Movements & Common Injuries) | Anatomy This video covers the anatomy of the elbow joint. We look visually at the three joints that make up the elbow, including their articulating surfaces, ligaments, synovial membrane, capsule, and bursae. Bones Involved in the Elbow Joint:• Humerus (humerus)• Radius (radius) – lateral bone of the forearm (thumb side)• Ulna (ulna) – medial bone of the forearm (pinky side) Joints within the Elbow Joint: Humeroulnar joint (articulatio humeroulnaris) • Classic hinge joint • Trochlea of humerus (trochlea humeri) + Trochlear notch of ulna (incisura trochlearis ulnae) • Allows flexion and extension Proximal radioulnar joint (articulatio radioulnaris proximalis) • Pivot joint • Articular circumference of radius (circumferentia articularis radii) + Radial notch of ulna (incisura radialis ulnae) • Enables pronation and supination Humeroradial joint (articulatio humeroradialis) • Ball-and-socket joint (functionally part of hinge system) • Capitulum of humerus (capitulum humeri) + Articular facet of radius (fovea articularis radii) Synovial Features & Capsule:• Synovial membrane (membrana synovialis) – surrounds all 3 joints in a single cavity• Fibrous capsule (capsula fibrosa) – encloses and stabilizes the joint• Sacciform recess (recessus sacciformis) – synovial fold over neck of radius to allow rotation Ligaments of the Elbow Joint:• Ulnar collateral ligament (ligamentum collaterale ulnare) • From medial epicondyle (epicondylus medialis) to ulna • Consists of anterior, posterior, and oblique bands • Stabilizes against valgus stress • Radial collateral ligament (ligamentum collaterale radiale) • From lateral epicondyle (epicondylus lateralis) • Blends with annular ligament • Annular ligament of radius (ligamentum anulare radii) • Encircles the head of radius and holds it in the radial notch • Allows pronation and supination • Quadrate ligament (ligamentum quadratum) • Short band between neck of radius and radial notch of ulna • Adds rotational stability Common Elbow Joint Injuries & Conditions:• Nursemaid’s elbow (radial head subluxation) – common in children• Olecranon bursitis – inflammation of the subcutaneous olecranon bursa• Valgus overload injuries – from throwing or trauma• Dislocation of the radial head – due to annular ligament weakness in toddlers• Elbow arthritis – affects the entire joint capsule due to shared synovial cavity Bursae of the Elbow Joint:• Subcutaneous olecranon bursa (bursa subcutanea olecrani) – between skin and olecranon (olecranon)• Subtendinous triceps bursa – beneath triceps tendon• Function: reduce friction during movement Movements of the Elbow Joint:• Flexion / Extension – at humeroulnar and humeroradial joints• Pronation / Supination – at proximal radioulnar joint Structures Mentioned in the Video:• Trochlea of humerus (trochlea humeri)• Capitulum of humerus (capitulum humeri)• Radial notch of ulna (incisura radialis ulnae)• Articular circumference of radius (circumferentia articularis radii)• Articular facet of radius (fovea articularis radii)• Olecranon of ulna (olecranon)• Medial epicondyle (epicondylus medialis)• Lateral epicondyle (epicondylus lateralis)• Neck of radius (collum radii)• Radial head (caput radii) Clinical Relevance Summary:• Joint stability maintained by ligaments and capsule• Joint motion involves coordinated action of all three articulations• Common injuries include ligament tears, bursitis, and nursemaid’s elbow• Ligaments and bursae are frequent sources of pain in overuse or trauma Sources:• Kozlowski, T. (2017). Memorix Anatomy, 2nd ed.• Standring S. (2020). Gray’s Anatomy, 42nd edition• Tubbs RS, Shoja MM, Loukas M. (2016). Bergman’s Encyclopedia of Human Anatomic Variation• White TD, Folkens PA. (2005). The Human Bone Manual Programs used: Complete Anatomy, Biorender, PowerPoint Transcript Introduction & Content0:00This is a video about the elbow joint. How it bends,0:03its articulations, and supporting structures. We are going to cover it by going through the0:07Joints within the elbow joint. It sounds weird but there are three
Shoulder Joint (Glenohumeral): Rotator Cuff, Capsule & Ligaments | Anatomy Explained
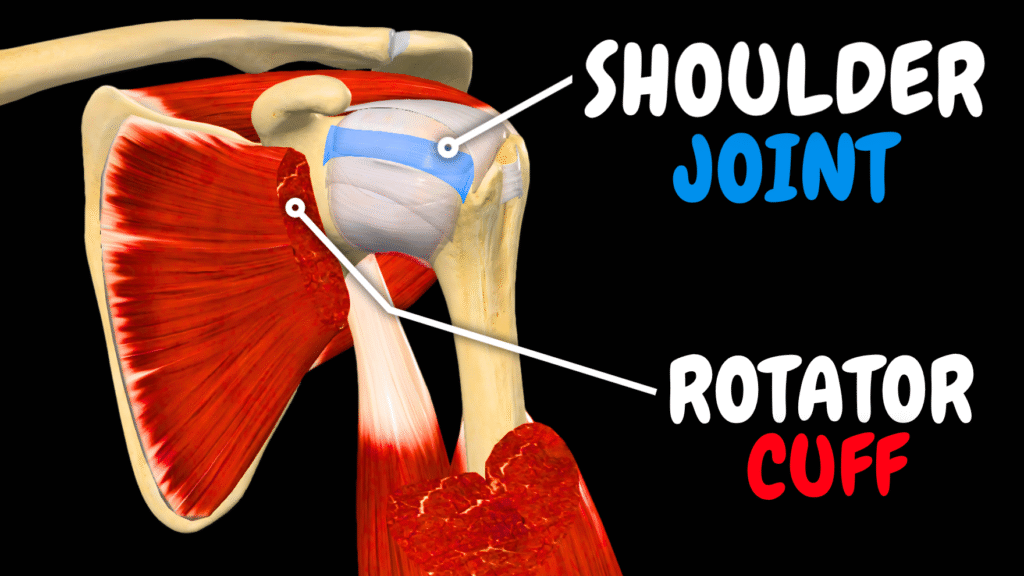
Shoulder Joint (Glenohumeral): Rotator Cuff, Capsule & Ligaments | Anatomy Explained Official Links Instagram Youtube Jki-discord Notes & Illustrations Quizzes Summary & Transcript The PDF for this topic is not available yetIt’s expected to be published by December 2025.In the meantime, test your knowledge using the QUIZ under the next tab! 12345678910 Shoulder Joint Test your understanding with 10 random multiple-choice questions from the question bank. You're in the preview mode. Note: All elements work correctly on the front end. 1 / 10 Which structure supports the biceps long head as it exits the capsule? A) Inferior glenohumeral ligament B) Coracohumeral ligament C) Middle glenohumeral ligament D) Transverse humeral ligament The transverse humeral ligament holds the tendon in the groove. 2 / 10 Which ligament helps hold the long head of the biceps tendon in place in the groove? A) Acromioclavicular ligament B) Coracohumeral ligament C) Inferior glenohumeral ligament D) Transverse humeral ligament The transverse humeral ligament stabilizes the tendon in the intertubercular groove. 3 / 10 Which tendon is most commonly involved in subacromial impingement? A) Biceps long head tendon B) Infraspinatus tendon C) Supraspinatus tendon D) Deltoid tendon The supraspinatus tendon is compressed under the acromion. 4 / 10 Where does the supraspinatus muscle insert? A) Coracoid process B) Greater tubercle of humerus C) Acromion D) Deltoid tuberosity It inserts on the greater tubercle of the humerus. 5 / 10 Which muscle initiates the first 15° of arm abduction? A) Teres minor B) Supraspinatus C) Deltoid D) Infraspinatus The supraspinatus is responsible for initial abduction. 6 / 10 Where does the infraspinatus muscle originate? A) Subscapular fossa B) Infraspinous fossa C) Supraspinous fossa D) Lateral border It arises from the infraspinous fossa of the scapula. 7 / 10 Which muscle originates from the lateral border of the scapula and externally rotates the arm? A) Teres minor B) Subscapularis C) Teres major D) Deltoid Teres minor arises from the lateral border and assists in external rotation. 8 / 10 What is the role of the intertubercular tendon sheath? A) Encases biceps tendon B) Prevents joint swelling C) Surrounds subscapularis D) Anchors deltoid It encases the biceps tendon in the groove and prevents friction. 9 / 10 What condition involves fibrosis of the axillary recess? A) Glenoid impingement B) Adhesive capsulitis C) Biceps tendinitis D) Shoulder bursitis Adhesive capsulitis causes stiffening of the shoulder capsule. 10 / 10 Which rotator cuff muscle decelerates the arm in overhead motion? A) Deltoid B) Teres major C) Infraspinatus D) Pectoralis major Infraspinatus is key in decelerating external rotation post-throw. Your score is The average score is 0% Description This video is about the shoulder joint.In this video, we break down all the anatomical structures that make and support the shoulder joint (bones, ligaments, bursae, rotator cuff muscles). Structures involved in the shoulder joint:Bones and Articular Surfaces:• Scapula – Flat, triangular bone forming the posterior base of the shoulder joint.• Humerus – Long bone of the upper arm; the head articulates with the glenoid cavity.• Clavicle – Acts as a strut between the sternum and scapula.• Glenoid cavity (Cavitas glenoidalis) – Shallow socket on the scapula that receives the head of the humerus.• Head of humerus (Caput humeri) – Ball-shaped proximal end of the humerus that articulates with the scapula.• Anatomical neck of humerus – Narrowing just below the humeral head; attachment site for the joint capsule.• Intertubercular groove (Sulcus intertubercularis) – Groove between the tubercles of the humerus for the biceps tendon. Labrum and Capsule:• Glenoid labrum (Labrum glenoidale) – Fibrocartilaginous rim that deepens the glenoid cavity for stability.• Articular capsule (Capsula articularis) – Encloses the joint and blends with periosteum.• Synovial membrane – Inner lining of the joint capsule that produces synovial fluid.• Fibrous capsule – Outer layer providing mechanical support.• Axillary recess – Inferior fold of the capsule allowing arm abduction. Glenohumeral Ligaments:• Superior glenohumeral ligament – Stabilizes the joint when the arm is at rest.• Middle glenohumeral ligament – Stabilizes during mid-range abduction and rotation.• Inferior glenohumeral ligament – Strongest, prevents anterior dislocation in abducted/externally rotated arm (ABER position).• Coracohumeral ligament – Supports the superior capsule, limits external rotation.• Transverse humeral ligament – Covers the bicipital groove and holds the biceps tendon in place. Coracoacromial Arch & Ligaments:• Coracoacromial ligament – Connects the coracoid process to the acromion, forming a superior arch.• Coracoacromial arch – Prevents upward displacement of the humeral head.• Acromioclavicular joint – Between clavicle and acromion; involved in arm elevation.• Coracoclavicular ligament – Anchors clavicle to scapula, indirect shoulder stabilizer. Rotator Cuff Muscles (Mnemonics SITS):• Supraspinatus – Initiates abduction; commonly involved in impingement.• Infraspinatus – External rotator, active in deceleration during throwing.• Teres minor – Assists with external rotation and stabilization.• Subscapularis – Primary internal rotator and anterior stabilizer. Other Muscles Mentioned:• Deltoid – Abducts the arm after supraspinatus initiates the movement.• Teres major – Assists with internal rotation and adduction.• Biceps brachii (long head) – Originates from supraglenoid tubercle; involved in shoulder stabilization. Tendons and Sheaths:• Long head of biceps tendon – Intracapsular, extrasynovial tendon that stabilizes the joint and is prone to tendinitis.• Intertubercular tendon sheath – Encloses the long head of biceps in the bicipital groove. Bursae of the Shoulder:• Subacromial bursa – Between acromion and supraspinatus tendon; inflamed in impingement.• Subdeltoid bursa – Cushions the deltoid muscle over the joint capsule.• Subtendinous bursa of teres major – Reduces friction under teres major.• Coracobrachial bursa – Lies beneath coracobrachialis muscle.• Coracoclavicular bursa – Found between coracoid process and clavicle.• Subcutaneous acromial bursa – Superficial, aids with overhead arm motion. Clinical Conditions Discussed:• Shoulder dislocation (especially anterior in ABER position)• SLAP tear (Superior Labrum Anterior Posterior lesion)• Rotator cuff tear (especially supraspinatus tendon)• Subacromial impingement syndrome• Frozen shoulder (Adhesive capsulitis)• Biceps tendinitis and instability• Shoulder pain during overhead activity• Weakness and limited range of motion due to cuff dysfunction Sources:• Kozlowski, T. (2017). Memorix Anatomy, 2nd ed.• Standring, S. (2020). Gray’s Anatomy, 42nd edition• Tubbs RS, Shoja MM, Loukas M. (2016). Bergman’s Encyclopedia of
Thoracic Joints: Costovertebral, Sternocostal & Rib Articulations | Anatomy
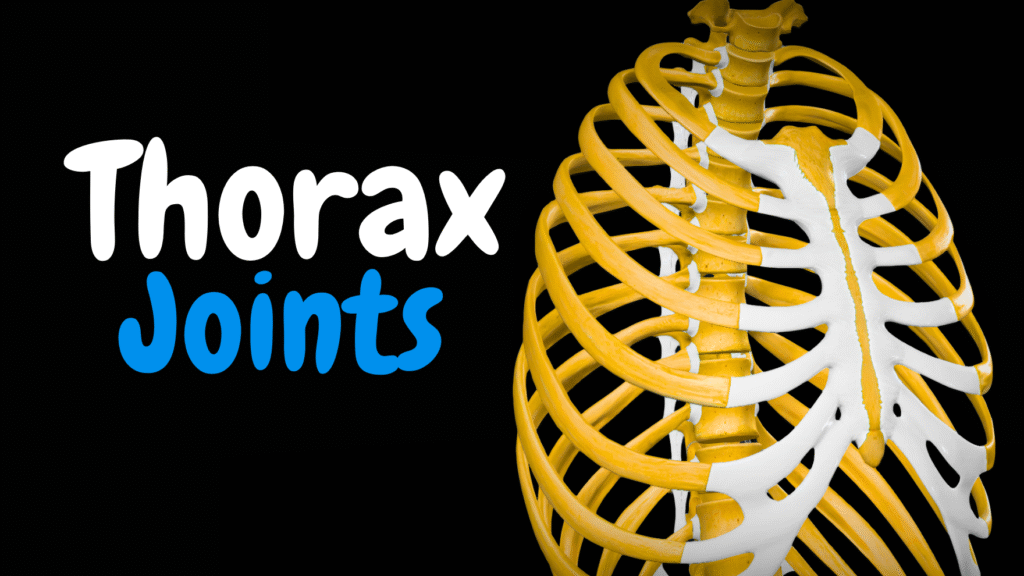
Thoracic Joints: Costovertebral, Sternocostal & Rib Articulations | Anatomy Official Links Instagram Youtube Jki-discord Notes & Illustrations Quizzes Summary & Transcript The PDF for this topic is not available yetIt’s expected to be published by December 2025.In the meantime, test your knowledge using the QUIZ under the next tab! 12345678910 Thoracic Joints Test your understanding with 10 random multiple-choice questions from the question bank. You're in the preview mode. Note: All elements work correctly on the front end. 1 / 10 What is the second synovial joint between rib and vertebra? A) Interchondral joint B) Sternocostal joint C) Costochondral joint D) Costotransverse joint The costotransverse joint connects rib tubercle and transverse process. 2 / 10 Which ligament spans from the rib neck to the vertebra above? A) Lateral costotransverse ligament B) Radiate ligament C) Superior costotransverse ligament D) Costotransverse ligament The superior costotransverse ligament attaches to the transverse process above. 3 / 10 Which membrane covers the external intercostal spaces anteriorly? A) Sternocostal membrane B) Internal intercostal membrane C) External intercostal membrane D) Costal periosteum The external intercostal membrane continues anteriorly from muscle fibres. 4 / 10 Which ligament reinforces the front of sternocostal joints? A) Costosternal ligament B) Sternal membrane C) Radiate sternocostal ligament D) Ligamentum nuchae The radiate sternocostal ligament fans from cartilage to sternum. 5 / 10 Which membrane covers the posterior intercostal spaces? A) External intercostal membrane B) Diaphragmatic fascia C) Internal intercostal membrane D) Costal ligament The internal intercostal membrane is the posterior continuation of the muscle. 6 / 10 What covers and stabilizes the anterior sternum region? A) Sternal membrane B) Supraspinous ligament C) Radiate ligament D) Costal cartilage The sternal membrane reinforces the sternocostal area. 7 / 10 What type of joints connect ribs 2–7 to the sternum? A) Synchondroses B) Syndesmoses C) Symphyses D) Synovial joints Ribs 2–7 form synovial sternocostal joints for flexibility in breathing. 8 / 10 Which ligament connects the rib head to the intervertebral disc ridge? A) Sternocostal ligament B) Costotransverse ligament C) Radiate ligament D) Intra‑articular ligament The intra‑articular ligament binds the crest of the rib head to the disc. 9 / 10 Why are interchondral joints clinically significant? A) Allow rib growth B) Cause scoliosis C) Harden costal cartilages D) Ossify with age They can ossify with age, reducing chest expansion. 10 / 10 Which ribs form costochondral joints with costal cartilage? A) Ribs 8–10 B) Ribs 11–12 C) Ribs 1–10 D) Ribs 1–7 Ribs 1–10 attach to cartilage via costochondral joints. Your score is The average score is 0% Description Joints of the Thoracic Cage (Ribs, Sternum & Vertebrae) | Anatomy Structures covered in this video: Joints Between Ribs and Vertebrae:• Joint of the head of the rib (Articulatio capitis costae) • Superior costal facet (Fovea costalis superior) • Inferior costal facet (Fovea costalis inferior) • Intervertebral disc (Discus intervertebralis) • Radiate ligament (Ligamentum capitis costae radiatum) • Intra-articular ligament (Ligamentum capitis costae intraarticulare)• Costotransverse joint (Articulatio costotransversaria) • Costotransverse ligament (Ligamentum costotransversarium) • Superior costotransverse ligament (Ligamentum costotransversarium superius) • Lateral costotransverse ligament (Ligamentum costotransversarium laterale) Joints Along the Rib Shaft:• Costochondral joints (Articulationes costochondrales)• Interchondral joints (Articulationes interchondrales) Associated Membranes and Muscles:• External intercostal membrane• Internal intercostal membrane• External intercostal muscles (Musculi intercostales externi)• Internal intercostal muscles (Musculi intercostales interni) Joints Between Ribs and Sternum:• Sternocostal joints (Articulationes sternocostales) – Ribs 2–7• First sternocostal joint – Synchondrosis (Synchondrosis sternocostalis prima)• Manubriosternal joint (Symphysis manubriosternalis)• Xiphisternal joint (Symphysis xiphosternalis) Supporting Structures:• Radiate sternocostal ligament (Ligamentum sternocostale radiatum)• Sternal membrane Movements and Function:• Rib cage expansion and contraction during respiration• Gliding movements at synovial joints• Stability and flexibility of thoracic wall• Protection of thoracic organs Clinical anatomy and conditions discussed:• Rib fracture and costotransverse pain• Thoracic stiffness with age (ossified interchondral joints)• Thoracic trauma and ligament injury• Use of sternal angle as a rib-counting landmark• Relevance of intercostal spaces in respiration Sources:• Kozlowski, T. (2017). Memorix Anatomy, 2nd ed.• Standring S. (2020). Gray’s Anatomy, 42nd edition• Tubbs RS, Shoja MM, Loukas M. (2016). Bergman’s Encyclopedia of Human Anatomic Variation• White TD, Folkens PA. (2005). The Human Bone Manual Programs used: Complete Anatomy, Biorender, PowerPoint Transcript Introduction & Content0:00In the previous videos we covered the bone anatomy of the vertebral column,0:04Ribs, and the sternum. Together, they form a solid cage around the heart and lungs. But the0:10thorax also needs to move with every breath you take, it expands and contracts with every breath.0:16To let that happen safely, that’s where the joints come in. They connect these0:19bones while still allowing flexibility. So the way we’re gonna cover them is by0:21first look at the joints between the ribs and the vertebral column back there. We’re gonna0:26look at the joints along the rib shaft, and the joints between the ribs and the sternum.0:30What’s up everyone, my name is Taim. I’m a medical doctor, and I make animated medical lectures to0:34make different topics in medicine visually easier to understand. If you’d like a PDF version or a0:39quiz of this presentation, you can find it on my website, along with organized video lectures0:43to help with your studies. Alright, let’s get started.Joints between Ribs and Vertebral Column0:46So let’s start with the joints between the ribs and the vertebral column. And for this,0:50let’s isolate the vertebra, two ribs, and look at the joints. In general, there are two major0:56joints here that we need to talk about, one is called the joint of the head of the rib,1:00and the other one is the costovertebral joint. Let’s look at this a little bit closer. The jointCostovertebral Joint1:06of the head of the rib is here. This is a synovial joint, and the articulating surfaces are the head1:12of the rib, which usually has two articular facets as you see here. These connect to the1:18superior costal facet of the vertebra below, and the inferior costal facet of the vertebra above,1:24with the intervertebral disc sitting between them. So, one rib head typically touches two vertebrae.1:31This setup gives the thoracic cage its stability but, this joint is actually supported by two main1:37ligaments. First, we have the radiate ligament. It spreads out from the
Vertebral Joints, Ligaments & Intervertebral Discs | Clinical Anatomy
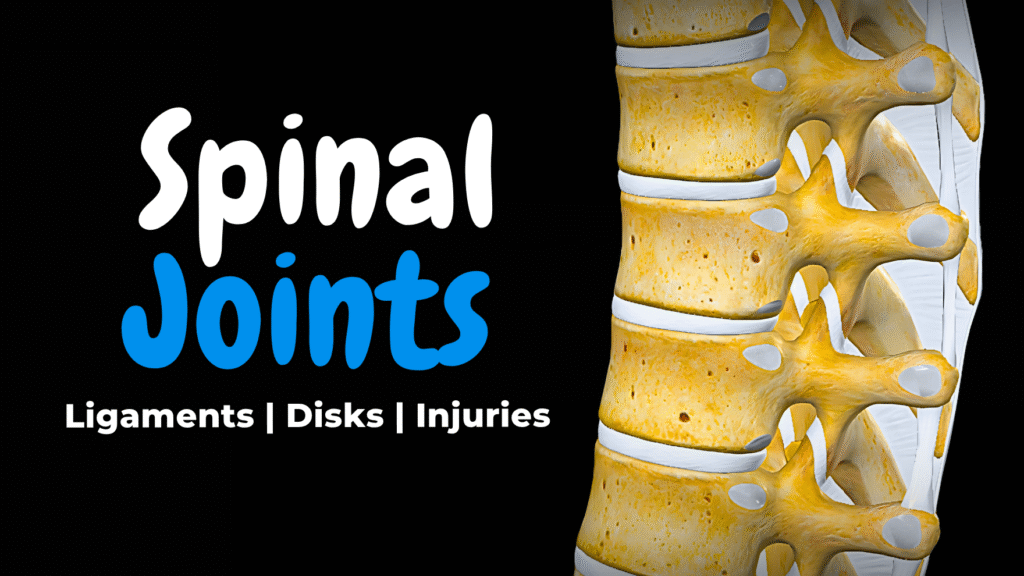
Vertebral Joints, Ligaments & Intervertebral Discs | Clinical Anatomy Official Links Instagram Youtube Jki-discord Notes & Illustrations Quizzes Summary & Transcript The PDF for this topic is not available yetIt’s expected to be published by December 2025.In the meantime, test your knowledge using the QUIZ under the next tab! 12345678910 Vertebral Joints Test your understanding with 10 random multiple-choice questions from the question bank. You're in the preview mode. Note: All elements work correctly on the front end. 1 / 10 What imaging is best to confirm lumbar disc herniation? A) CT scan B) X-ray C) MRI D) Ultrasound MRI provides clear images of soft tissues like discs and nerves. 2 / 10 Which ligament runs along the anterior surfaces of vertebral bodies? A) Anterior longitudinal ligament B) Supraspinous ligament C) Ligamentum flavum D) Posterior longitudinal ligament The anterior longitudinal ligament prevents hyperextension. 3 / 10 What is the structure that thickens to become the nuchal ligament? A) Alar ligament B) Supraspinous ligament C) Interspinous ligament D) Transverse ligament The supraspinous ligament thickens in the neck to form nuchal ligament. 4 / 10 What movement is allowed by the median atlanto‑axial joint? A) Extension B) Rotation C) Flexion D) Abduction The pivot joint allows head rotation (“no” movement). 5 / 10 What structure forms the roof of the vertebral canal? A) Vertebral bodies B) Transverse processes C) Laminae D) Spinous processes The laminae of vertebrae form the posterior roof of the canal. 6 / 10 What is a feature of plane synovial joints in the spine? A) Flexion-extension only B) Hinge rotation C) Gliding movement D) Fused mobility Zygapophysial joints allow gliding between vertebrae. 7 / 10 Which ligament holds the dens against the atlas? A) Alar ligament B) Nuchal ligament C) Transverse ligament of atlas D) Posterior longitudinal ligament The transverse ligament secures the dens at median joint. 8 / 10 Which membrane lies posterior to the foramen magnum and connects to C1? A) Alar ligament B) Supraspinous ligament C) Anterior atlanto-occipital membrane D) Posterior atlanto-occipital membrane The posterior atlanto-occipital membrane connects occiput to atlas. 9 / 10 At which spinal level did the MRI indicate a herniation in the case example? A) C6/C7 B) T12/L1 C) L4/L5 D) L5/S1 The herniation was at L5/S1 compressing the S1 root. 10 / 10 Which ligament runs between spinous processes along the midline? A) Supraspinous ligament B) Intertransverse ligament C) Interspinous ligament D) Ligamentum flavum Supraspinous ligament connects spinous tips. Your score is The average score is 0% Description Structures covered in this video: Fibrous Joints (Syndesmoses):• Anterior longitudinal ligament (Ligamentum longitudinale anterius)• Posterior longitudinal ligament (Ligamentum longitudinale posterius)• Anterior sacrococcygeal ligament (Ligamentum sacrococcygeum anterius)• Superficial posterior sacrococcygeal ligament (Ligamentum sacrococcygeum posterius superficiale)• Ligamenta flava (Ligamenta flava)• Intertransverse ligaments (Ligamenta intertransversaria)• Interspinous ligaments (Ligamenta interspinalia)• Supraspinous ligament (Ligamentum supraspinale)• Nuchal ligament (Ligamentum nuchae) Cartilaginous Joints (Symphyses):• Intervertebral disc (Discus intervertebralis)• Annulus fibrosus (Anulus fibrosus)• Nucleus pulposus (Nucleus pulposus)• Lumbosacral symphysis (Symphysis lumbosacralis)• Sacrococcygeal symphysis (Symphysis sacrococcygea) Synovial Joints:• Zygapophysial joints / Facet joints (Articulationes zygapophysiales)• Lateral atlanto-axial joints (Articulationes atlantoaxiales laterales)• Median atlanto-axial joint (Articulatio atlantoaxialis mediana)• Atlanto-occipital joint (Articulatio atlantooccipitalis)• Posterior atlanto-occipital membrane (Membrana atlantooccipitalis posterior)• Anterior atlanto-occipital membrane (Membrana atlantooccipitalis anterior)• Lateral atlanto-occipital ligament (Ligamentum atlantooccipitale laterale)• Transverse ligament of atlas (Ligamentum transversum atlantis) Bony Joints (Synostoses):• Sacral vertebral fusion (Synostoses of vertebrae sacrales)• Coccygeal vertebral fusion (Synostoses of vertebrae coccygeae) Clinical anatomy and conditions discussed:• Disc herniation (Herniated disc)• Sciatica (Nerve root compression at L5/S1)• Facet joint arthropathy• Rheumatoid arthritis affecting the transverse ligament• Atlantoaxial instability• Degeneration of intervertebral discs• Nerve root compression symptoms (pain, numbness, weakness) Movements enabled by vertebral joints:• Flexion• Extension• Lateral flexion• Rotation Function of vertebral joints and ligaments:• Stability of vertebral column• Protection of spinal cord and nerve roots• Shock absorption• Controlled mobility• Prevention of hyperextension and hyperflexion Sources:• Kozlowski, T. (2017). Memorix Anatomy, 2nd ed.• Standring S. (2020). Gray’s Anatomy, 42nd edition.• Tubbs RS, Shoja MM, Loukas M. (2016). Bergman’s Encyclopedia of Human Anatomic Variation• White TD, Folkens PA. (2005). The Human Bone Manual Programs used: Complete Anatomy, Biorender, PowerPoint Transcript Introduction & Content0:00In the last video, we covered the bones of the spine. Today, we’ll learn about the joints,0:05ligaments, and discs. How they hold the spine together, and how injury to those structures0:10can result in pain, herniation, and instability. So in this video we’ll start with the why do we0:15have vertebral joints, how are the vertebral joints structured and how do we classify them?0:21The vertebral joints are well organized and it makes so much sense once you know fibrous joints,0:27cartilagionous joints, synovial joints and the bony joints. So that’s our goal for today,0:32understanding all of these joints, and also look specifically at common0:36injuries like disk herniations as well. What’s up everyone, my name is Taim. I’m0:40a medical doctor, and I make animated medical lectures to make different topics in medicine0:44visually easier to understand. If you’d like a PDF version or a quiz of this presentation, you can0:49find it on my website, along with organized video lectures to help with your studies.0:53Alright, let’s get started. Why, How, Classification.Why do we have vertebral joints?0:57Why do we have vertebral joints? I think this is one of the things that really makes1:01you appreciate the structure of the spine. If the vertebrae were fused together into a single bone,1:07we wouldn’t be able to move properly. The vertebral joints allow flexibility and movement,1:12making it possible for the spine to bend forward in flexion, bend backward in extension,1:18and rotate along its axis. At the same time, they maintain spinal stability and keep the vertebrae1:24properly aligned, so the spine doesn’t collapse under its own weight. Another important role of1:29the vertebral joints is protecting the spinal cord and the spinal nerves during movement, by keeping1:34the vertebral canal stable and minimizing any compression or stretching. They also help absorb1:41and distribute mechanical forces, especially when we walk, run, or lift — so that the forces don’t1:47damage the bones or nerves. And they also enable coordinated movements of the head and trunk,1:53allowing
Skull Joints: Fontanelles, Sutures, TMJ & Synchondroses | Anatomy
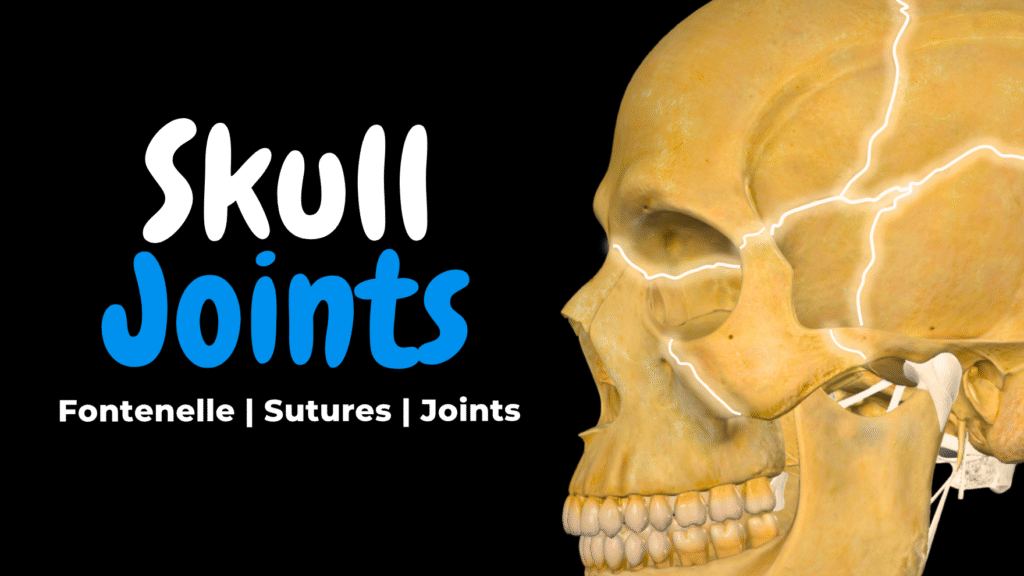
Skull Joints: Fontanelles, Sutures, TMJ & Synchondroses | Anatomy Official Links Instagram Youtube Jki-discord Notes & Illustrations Quizzes Summary & Transcript Notes ☆ Members Only Go to PDF Notes Illustrations ☆ Members Only Go to Illustrations 12345678910 Skull Joints – QUIZ Test your understanding with 10 random multiple-choice questions from the question bank. You're in the preview mode. Note: All elements work correctly on the front end. 1 / 10 Which ligament limits posterior displacement of the mandible in the TMJ? A) Stylomandibular ligament B) Pterygospinous ligament C) Lateral temporomandibular ligament D) Articular capsule The lateral temporomandibular ligament stabilizes the joint. 2 / 10 What type of joint is a skull suture in adults? A) Synarthrosis B) Diarthrosis C) Amphiarthrosis D) Synchondrosis Skull sutures are fibrous, immovable joints—synarthroses. 3 / 10 Which of the following is a major difference between the newborn and adult skull? A) Fixed mandible B) Fully fused sutures C) Smaller viscerocranium D) Larger paranasal sinuses In newborns, the viscerocranium is much smaller relative to the neurocranium. 4 / 10 What does a bulging fontanelle in a non-crying baby usually indicate? A) Dehydration B) Increased intracranial pressure C) Fontanelle ossification D) Normal development It may suggest increased intracranial pressure. 5 / 10 Which synchondrosis typically ossifies by age 18–25? A) Sphenoethmoidal synchondrosis B) Sphenomandibular synchondrosis C) Spheno-occipital synchondrosis D) Petro-parietal synchondrosis The spheno-occipital synchondrosis ossifies in late adolescence. 6 / 10 What movement occurs in the lower compartment of the TMJ? A) Medial shift B) Hinge-like rotation C) Lateral gliding D) Protrusion The lower compartment allows hinge movement like opening the mouth. 7 / 10 What is the anterior fontanelle’s usual closure time? A) 2–6 weeks B) 5–7 months C) 12–24 months D) 6 years The anterior fontanelle closes between 12 and 24 months. 8 / 10 What structure divides the TMJ into two synovial compartments? A) Meniscus B) Articular cartilage C) Synovial capsule D) Articular disc The articular disc separates the superior and inferior compartments. 9 / 10 At birth, the face-to-cranium ratio is approximately: A) 1:01 B) 1:04 C) 1:08 D) 01:03.0 The facial bones are small in neonates. 10 / 10 What is the primary function of fontanelles in the newborn skull? A) To allow brain growth and flexibility B) To produce bone marrow C) To anchor facial muscles D) To protect sinuses Fontanelles allow flexibility during birth and brain growth after birth. Your score is The average score is 0% Description Structures covered in this video:• Fontanelles (Fonticuli cranii):– Anterior fontanelle (Fonticulus anterior)– Posterior fontanelle (Fonticulus posterior)– Sphenoid (anterolateral) fontanelle (Fonticulus sphenoideus)– Mastoid (posterolateral) fontanelle (Fonticulus mastoideus) • Sutures (Suturae cranii):– Coronal suture (Sutura coronalis)– Sagittal suture (Sutura sagittalis)– Lambdoid suture (Sutura lambdoidea)– Squamous suture (Sutura squamosa)– Parietomastoid suture (Sutura parietomastoidea)– Sphenosquamous suture (Sutura sphenosquamosa)– Frontal suture / Metopic suture (Sutura frontalis)– Persistent frontal suture (Sutura frontalis persistens) • Synarthroses (immovable joints):– Sutures (Suturae cranii)– Synchondroses (Synchondroses cranii):• Sphenopetrosal synchondrosis (Synchondrosis sphenopetrosa)• Petro-occipital synchondrosis (Synchondrosis petrooccipitalis)• Spheno-occipital synchondrosis (Synchondrosis sphenooccipitalis)• Sphenoethmoidal synchondrosis (Synchondrosis sphenoethmoidalis)– Gomphoses (Gomphoses dentales):• Root of tooth (Radix dentis)• Alveolar socket (Alveolus dentalis)• Periodontal ligament (Ligamentum periodontale) • Temporomandibular Joint (Articulatio temporomandibularis):– Condylar process of mandible (Processus condylaris mandibulae)– Mandibular fossa of temporal bone (Fossa mandibularis ossis temporalis)– Articular disc (Discus articularis)– Superior synovial cavity (Cavitas synovialis superior)– Inferior synovial cavity (Cavitas synovialis inferior)– Articular capsule (Capsula articularis)– Lateral temporomandibular ligament (Ligamentum temporomandibulare laterale)– Sphenomandibular ligament (Ligamentum sphenomandibulare)– Stylomandibular ligament (Ligamentum stylomandibulare) • Accessory ligaments and fibrous structures:– Stylohyoid ligament (Ligamentum stylohyoideum)– Pterygospinous ligament (Ligamentum pterygospinosum)– Pterygomandibular raphe (Raphe pterygomandibularis) • Bones referenced for orientation:– Frontal bone (Os frontale)– Parietal bone (Os parietale)– Occipital bone (Os occipitale)– Temporal bone (Os temporale)– Sphenoid bone (Os sphenoidale)– Ethmoid bone (Os ethmoidale)– Maxilla (Maxilla)– Mandible (Mandibula)– Zygomatic bone (Os zygomaticum) Clinical anatomy and conditions discussed:• Dehydration and sunken fontanelle• Hydrocephalus and bulging fontanelle• Meningitis and increased intracranial pressure• Delayed closure of anterior fontanelle (congenital hypothyroidism, rickets, Down syndrome)• Early closure of fontanelles and sutures (craniosynostosis)• Persistent frontal suture (Sutura frontalis persistens)• TMJ dysfunctions and ligament injuries• Nerve compression from ossified pterygospinous ligament (Civinini’s foramen and mandibular nerve compression) Transcript 0:00You are born with gaps in your skull. It sounds strange, but there’s a very logical reason for it.0:06These gaps allow the skull to stay flexible during birth and give space for the brain to grow during0:11early development. We call them fontanelles, and this is what we call the developing skull.0:17As the child grows, those gaps slowly close, and the skull begins to form joints. Most0:23of these joints become completely stiff called sutures. Others, become a movable0:28joint that allows the jaw to move freely. In this video, we’ll first look at theContent0:33developing skull, go through the fontanelles, and highlight the differences between a newborn and0:37an adult skull. Then I’ve made it very logical to understand the joints of the adult skull, and that0:43is by dividing them into two types. The immovable joints, or synarthroses, including sutures,0:50synchondroses, and gomphoses, and the one movable joint, the temporomandibular joint. We will cover0:56each of these and put in a few clinical notes along the way to make it interesting.1:01What’s up everyone, my name is Taim. I’m a medical doctor, and I make animated medical lectures to1:05make different topics in medicine visually easier to understand. If you’d like a PDF version or a1:10quiz of this presentation, you can find it on my website, along with organized video lectures1:14to help with your studies. Alright, let’s get started.The Developing Skull1:16So let’s start with the developing skull. Let’s start by adding a newborn skull and an adult1:22skull. The newborn skull on the left represents about 0-1 months old, and the adult skull around1:2825 years old. What happens is, at birth, the bones of the skull are not fully fused. Instead,1:35they’re connected by soft connective tissue, forming what we call the fontanelles. And I’ll1:40touch upon that in more details in a minute, but these allow for flexibility during birth,1:45and also leave space for the brain to grow rapidly in the first
What Are Joints? Classification, Types & Clinical Anatomy Explained
What Are Joints? Classification, Types & Clinical Anatomy Explained Official Links Instagram Youtube Jki-discord Notes & Illustrations Quizzes Summary & Transcript Notes ☆ Members Only Go to PDF Notes Illustrations ☆ Members Only Go to Illustrations 12345678910 Joints Overview – QUIZ Test your understanding with 10 random multiple-choice questions from the question bank. You're in the preview mode. Note: All elements work correctly on the front end. 1 / 10 What fluid reduces friction inside a synovial joint? A) Serous fluid B) Perilymph C) Synovial fluid D) Interstitial fluid Synovial fluid lubricates and nourishes the joint. 2 / 10 What is the primary purpose of joints in the body? A) To connect bones and allow movement B) To attach tendons C) To generate force D) To transmit blood Joints link bones together and allow varying degrees of movement. 3 / 10 What are bursae? A) Joint capsules B) Fluid-filled sacs reducing friction C) Articular discs D) Shock-absorbing pads Bursae are fluid-filled sacs that reduce friction in joints. 4 / 10 Which of the following joints is a temporary cartilaginous joint during development? A) Epiphyseal growth plate B) Glenohumeral joint C) Intervertebral disc D) Pubic symphysis Epiphyseal plates are synchondroses that ossify over time. 5 / 10 What kind of movement is allowed by amphiarthroses? A) Multiplanar mobility B) Free rotation C) No movement D) Slight movement Amphiarthroses allow slight movement; they’re often cartilaginous. 6 / 10 What connective tissue structure surrounds and stabilizes a synovial joint? A) Ligaments B) Articular cartilage C) Articular capsule D) Synovial membrane The fibrous articular capsule maintains structural integrity. 7 / 10 Which structure connects bone to bone in a joint? A) Labrum B) Tendons C) Ligaments D) Menisci Ligaments stabilize joints by connecting bones. 8 / 10 What cartilage type makes up symphyses? A) Elastic cartilage B) Articular cartilage C) Fibrocartilage D) Hyaline cartilage Symphyses consist of fibrocartilage. 9 / 10 What type of joint is found between the atlas and axis (C1–C2)? A) Saddle B) Plane C) Pivot D) Ellipsoid The atlantoaxial joint is a pivot joint that allows rotation. 10 / 10 Which of the following is true about the hip joint? A) Allows only flexion and extension B) Has an acetabular labrum C) Is a hinge joint D) Is a saddle joint The acetabular labrum deepens the socket and stabilizes the hip joint. Your score is The average score is 0% Description This video is about joint classification, structure, function, and clinical relevance. Topics covered in this video: • What are joints?• Joint classification based on structure and function• Types of joints in the human body• Examples of fibrous, cartilaginous, and synovial joints• Subtypes of each joint category with real anatomical examples• Clinical relevance of joints (e.g., high ankle sprains, TMJ, arthritis)• Supporting structures: ligaments, bursae, menisci, labrum, fat pads• Functional mobility: synarthrosis, amphiarthrosis, diarthrosis• Synovial joint types: – Ball-and-socket joint (shoulder, hip) – Ellipsoid joint (wrist) – Saddle joint (thumb) – Hinge joint (elbow, knee, fingers) – Pivot joint (atlantoaxial, radioulnar) – Plane joint (acromioclavicular, vertebral facet joints) Joint classification explained:• Fibrous joints – sutures (suturae), syndesmoses, gomphoses• Cartilaginous joints – synchondroses (hyaline cartilage), symphyses (fibrocartilage)• Synovial joints – contain a joint cavity filled with synovial fluid – include articular cartilage, synovial membrane, joint capsule – supported by ligaments, tendons, labrum, bursae, menisci Clinical anatomy references include:• Atlantoaxial joint (articulatio atlantoaxialis mediana)• Glenohumeral joint (articulatio humeri)• Temporomandibular joint (articulatio temporomandibularis)• Proximal radioulnar joint (articulatio radioulnaris proximalis)• Pubic symphysis (symphysis pubica)• Costochondral joints (junctiones costochondrales)• Intervertebral discs (disci intervertebrales)• Distal tibiofibular syndesmosis (syndesmosis tibiofibularis distalis) Whether you’re a medical student or revising anatomy for clinical practice, this video breaks down complex arthrology in a visual, memorable way. Transcript 0:00Joints. They come in many forms, but at their core, joints exist to link bones0:05together and allow movement. Some let you rotate your arm in every direction,0:10some move just a little bit, and some, like the joints in your skull, don’t move at all.0:16You don’t really think about them, until something goes wrong. When joints wear down,0:21become inflamed, or stop working properly, even the simplest movements can become difficult.0:27So, why are some joints flexible while others are completely rigid? What makes0:32one joint allow movement while another barely moves at all? And how do we actually classify0:38all the different joints in the body? In this video, we’ll start by answering0:43the fundamental question – what are joints? Then, we’ll go through all the joints in the body and0:49classify them based on their structure and function. As we go through them,0:54we’ll also highlight their clinical relevance, understanding how joint problems develop and0:58what makes them vulnerable to damage. Hey everyone, my name is Taim. I’m a1:02medical doctor, and I make animated medical lectures to make different topics in medicine1:06visually easier to understand. If you’d like a PDF version or a quiz of this presentation, you can1:11find it on my website, along with organized video lectures to help with your studies.1:15Alright, let’s get started! So what are joints?What are Joints?1:19Just, in simple terms, The point at which two bones lay adjacent to each1:24other (with or without the ability to move) is called a joint. Let’s visualize this.1:30Here we see a bone. Here is another bone. The point at which they lay adjacent to1:35each other is a joint. Here are two bones, between them, a joint. Here are two bones,1:41between them a joint. And even, I’ll surprise you now. Even between your skull bones, is a joint.1:48So joints come in different shape, and they are structurally and functionally different.1:54For example. The shoulder joint is1:56called the glenohumeral joint. Structurally, we call this a Synovial joint, Functionally,2:02it’s a Diarthrosis, since it’s a freely movable joint. And we subclassify it as a ball-and-socket2:09joint, which provides free rotational movement. Between the articular surfaces of vertebrae,2:15we got the facet joint, or zygapophyseal joints. They are synovial joints,2:20functionally movable so diarthrosis as well, but subclassified as plane joint,2:26allowing only gliding movements. Okay, let’s take another example, in the skull we got2:32sutures. Or lambdoid suture is what we’re pointing at specifically now. Structurally,2:37it’s